Parkinsonism
A 33 YR MALE FLOWER POT MAKER BY OCCUPATION RESIDENT OF BONAGIRI CAME TO OPD WITH
CHIEF COMPLAINT:-
Abnormal movements in his upper limbs since 5 years.
Difficulty in walking since 5 years.
HOPI:-
The patient is apparently asymptomatic 5 years back then he started developing abnormal involuntary movements in his upper limbs since 5 years. The movements were noticed during rest and also while walking.
Patient also complaints of difficulty in walking in the form of difficulty in initiation and once he walks, he walks with short sride length and freezes during turning.
There is also decreased swinging of hands while walking.
Difficulty in speaking.
he is able to appreciate smell,
hes able to look towards all sides
no h/o sensory loss over the face,
no facial deviation
No h/o auditory disturbances
No h/o restricted tongue movements
No difficulty in swallowing
No h/o abnormal sweating
No h/o shooting pain
No h/o headache or vomiting.
No h/o seizures
PAST HISTORY:-
K/c/o schizophrenia since 2006 and he used anti-psychotics.
N/k/c/o DM , HTN ,ASTHMA, TB, EPILEPSY.
TREATMENT HISTORY:-
Used anti-psychotics.

DAILY ROUTINE:-

FAMILY HISTORY:-
No significant family history.
PERSONAL HISTORY:-
MARITAL STATUS:- Married
DIET:-Mixed
APPETITE:-NORMAL
SLEEP:- regular and adequate
Bowel and bladder:- regular
No history of any allergens
No addictions
GENERAL EXAMINATION:-
Patient is conscious, coherent, cooperative
moderately built and moderately nourished
No Pallor Icterus cyanosis clubbing Lymphadenopathy Edema
VITALS :
Temp: Afebrile
PR: 80 bpm
Rr:16 cycles /min
BP: 110/60 mm of hg



SYSTEMIC EXAMINATION : -
RESPIRATORY SYSTEM : -
Trachea Central
NVBS
CVS :-
S1 and s2 sounds heard
No cardiac murmurs
ABDOMINAL EXAMINATION :
shape - scaphoid
Palpable mass - no
Liver - not palpable
Spleen - not palpable
Bowel sounds - normal
NEUROLOGICAL EXAMINATION :
Higher mental function
The patient is conscious well oriented to time, place and person.
No delusions or hallucinations
Cranial nerve examination:-
CN1:- smell sense RIGHT LEFT
+ +
CN2:- visual acuity normal Normal
CN3,4,6:- extra ocular movement : full and free in all directions.
Direct light reflex :-present
Consensual light reflex :-present
Ptosis :- absent
Accommodation reflex :-present
CN5:- Sensory : over face ,buccal mucosa : normal
Motor: masseter ,temporalis : normal
Reflexes :corneal : normal
Conjunctival : normal
CN7:- Motor : nasolabial fold : present
Reflexes: corneal conjunctival present
CN8:- Rinnes:- +
Webers:- not lateralised
Nystagmus :- absent
CN9 ,10 :- uvula movements normal
Motor system:
BULK: Inspection : normal
Palpation : normal
MID ARM CIRCUMFERENCE:
Upper limb R L
Proximal muscles. 24cm. 24cm
Distal muscles 25cm 25cm
Lower limb R L
Proximal muscles. 36cm. 36cm
Distal muscles 29cm 30cm
TONE: both upper limbs:- rigid while extension of the elbow joint( LEAD PIPE)
both lower limbs- normal
POWER:
Elbow:
Flexion. 4/5. 4/5
Extension: 4/5. 4/5
Wrist:
Flexion:4/5. 4/5
Extension: 4/5. 4/5
Abduction : 4/5. 4/5
adduction:4/5. 4/5
Hand grip:- good
HIP:-
Flexion:4/5. 4/5
Extension. 4/5. 4/5
Knee :-
Flexion 4-/5. 4-/5
Extension. 4/5. 4/5
Plantarflexion:. 4/5. 4/5
Dorsiflexion. 4/5. 4/5
Toe. 4/5 4/5
Reflexes :
SUPERFICIAL:
Present
DEEP TENDON REFLEXES :
Rt Lft
Biceps : + 1 +1
Triceps: +1 +1
Supinator: +1 +1
Knee jerk: +2 +2
Ankle jerk: +1 +1
Involuntary activities:-
https://youtube.com/shorts/6mLEcJBz_Bk?feature=share3
GAIT:-
SENSORY SYSTEM :
Posterior column:
fine touch - normal
Vibration - normal
SPINO THALAMIC :
Pain : present
Temperature: present
Crude touch - normal
CEREBELLAR SIGNS :
Finger nose test : normal
Heel knee test : able to do
Dysdiadokinesia- absent
Romberg test - negative
MENINGEAL SIGNS
neck stiffnesses. Absent
Kernigs sign - absent
Brudzinski sign - not visualised
Drawing a circle:-

Investigations:-

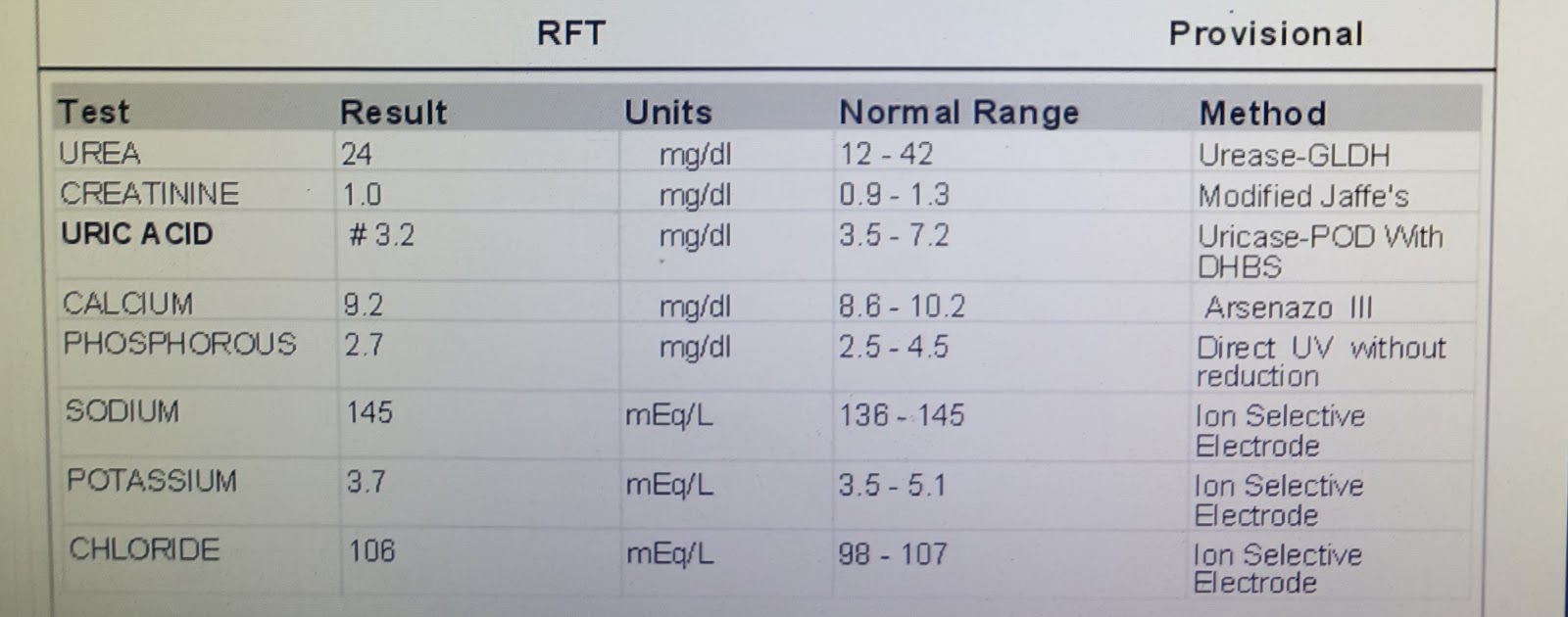













Comments